Gums
Gums or gingiva are part of the soft tissue lining of the mouth. They surround the teeth and provide a seal around them. Compared with the soft tissue linings of the lips and cheeks, most of the gums are tightly bound to the underlying bone which helps resist the friction of food passing over them.
Anatomy[edit]
The gums are divided into two main areas: the attached gingiva and the unattached or free gingiva. The attached gingiva is tightly bound to the underlying bone and the cementum of the root surface to provide a seal around the tooth. The free gingiva forms the soft wall of the gingival sulcus.
Health and disease[edit]
Healthy gums are usually coral pink, but may contain melanin, making them appear darker. Changes in color, particularly increased redness, together with swelling or bleeding of the gums, can be signs of gum disease.
Gum disease is a common condition where the gums become swollen, sore or infected. It's estimated to affect more than half of all adults in the UK to some degree and most people experience it at least once. It's much less common in children.
If gum disease is treated in its early stages, it's completely reversible. If it's not treated, a condition called periodontitis can develop. This can lead to loss of teeth.
Prevention and treatment[edit]
Good oral hygiene and regular dental examinations are the best way to prevent gum disease. The main treatment for gum disease is a professional clean to remove the build-up of plaque and tartar. This can be done by a dentist or dental hygienist.

This WikiMD article can only be edited by registered and verified editors. You can log in or register.
Gums gallery[edit]
-
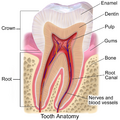 Tooth Anatomy
Tooth Anatomy -
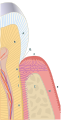 Periodontium
Periodontium -
Hyperpigmentation of the Gum



Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian

{kind=link}