Macrolide
Macrolide is a class of antibiotics that are used in the treatment of various bacterial infections. They are derived from Streptomyces bacteria. Macrolides work by inhibiting protein synthesis in bacteria, preventing them from growing and reproducing.
History[edit]
The first macrolide, Erythromycin, was discovered in the 1950s. Since then, several other macrolides have been developed, including Clarithromycin and Azithromycin.
Mechanism of action[edit]
Macrolides bind to the 50S subunit of the bacterial ribosome, inhibiting the translocation of peptidyl-tRNA. This prevents the addition of new amino acids to the growing peptide chain, effectively stopping protein synthesis.
Uses[edit]
Macrolides are used to treat a variety of bacterial infections, including respiratory tract infections, skin infections, and sexually transmitted infections. They are also used in patients who are allergic to penicillin.
Side effects[edit]
Common side effects of macrolides include nausea, vomiting, diarrhea, and abdominal pain. In rare cases, they can cause serious side effects like hepatotoxicity and cardiac arrhythmias.
Resistance[edit]
Bacterial resistance to macrolides is a growing concern. Resistance can occur through several mechanisms, including mutation of the 50S ribosomal subunit and efflux of the antibiotic out of the bacterial cell.
See also[edit]

This WikiMD article can only be edited by registered and verified editors. You can log in or register.
-
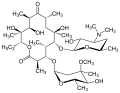 Erythromycin structure
Erythromycin structure -
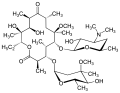 Clarithromycin structure
Clarithromycin structure -
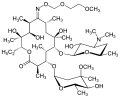 Roxithromycin structure
Roxithromycin structure -
Azithromycin 250mg tablets



Sponsored Health Resource

W8MD Weight Loss, Sleep & MedSpa
Looking for physician-supervised weight loss, semaglutide, tirzepatide, or GLP-1 receptor agonist options? W8MD helps eligible patients in New York City, Brooklyn, New Jersey, Connecticut, Pennsylvania, Delaware, and greater Philadelphia with medical weight loss, sleep medicine, and long-term maintenance support.
GLP-1 specials: Affordable GLP-1 injections NYC and Philadelphia starting from $29.99/week and up for semaglutide with insurance accepted for qualifying visits, and $45/week and up for tirzepatide with insurance accepted for qualifying visits. Self-pay options start from $59.99/week and up for semaglutide and $69.99/week and up for tirzepatide.
- Medical weight loss NYC
- Affordable GLP-1 injections NYC
- Budget GLP-1 weight loss shots Philadelphia
- New Jersey medical weight loss
- NYC medical weight loss blog
- Philadelphia weight loss blog
- Sleep medicine and sleep apnea services
- W8MD MedSpa and wellness
Book a W8MD appointment · View GLP-1 specials
Paid promotional message. Eligibility, pricing, insurance coverage, medication availability, and results vary. Medical evaluation required.

Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian

{kind=link}