Alpha-mannosidosis
| Alpha-mannosidosis | |
|---|---|
| Synonyms | N/A |
| Pronounce | N/A |
| Specialty | N/A |
| Symptoms | Intellectual disability, hearing loss, skeletal abnormalities |
| Complications | N/A |
| Onset | Childhood |
| Duration | Lifelong |
| Types | N/A |
| Causes | Genetic mutation in the MAN2B1 gene |
| Risks | N/A |
| Diagnosis | Genetic testing, clinical evaluation |
| Differential diagnosis | N/A |
| Prevention | N/A |
| Treatment | Enzyme replacement therapy, hematopoietic stem cell transplantation |
| Medication | N/A |
| Prognosis | Variable |
| Frequency | Rare |
| Deaths | N/A |
Alpha-mannosidosis is a rare genetic disorder characterized by the body's inability to properly break down certain complex sugars due to a deficiency of the enzyme alpha-mannosidase. This condition is classified as a lysosomal storage disorder.
Signs and Symptoms[edit]
Individuals with alpha-mannosidosis may exhibit a range of symptoms, including intellectual disability, hearing loss, and skeletal abnormalities. Other common features include immune system deficiencies, facial dysmorphism, and motor function impairment. Symptoms typically appear in childhood and can vary in severity.
Causes[edit]
Alpha-mannosidosis is caused by mutations in the MAN2B1 gene, which provides instructions for producing the enzyme alpha-mannosidase. This enzyme is essential for the breakdown of oligosaccharides in the lysosome. Mutations in the MAN2B1 gene lead to a deficiency of this enzyme, resulting in the accumulation of undigested sugars in the body's cells.
Diagnosis[edit]
Diagnosis of alpha-mannosidosis is based on clinical evaluation and confirmed through genetic testing. Biochemical tests may also be used to measure the activity of the alpha-mannosidase enzyme in blood or tissue samples.
Treatment[edit]
Currently, treatment options for alpha-mannosidosis include enzyme replacement therapy and hematopoietic stem cell transplantation. These treatments aim to reduce symptoms and improve quality of life. Supportive therapies, such as physical therapy and speech therapy, may also be beneficial.
Prognosis[edit]
The prognosis for individuals with alpha-mannosidosis varies depending on the severity of the condition and the effectiveness of treatment. Early diagnosis and intervention can improve outcomes and quality of life.
See Also[edit]
References[edit]
External Links[edit]
- Genetic and Rare Diseases Information Center
- Orphanet
Alpha-mannosidosis[edit]
-
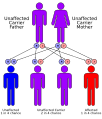 Autosomal recessive inheritance pattern
Autosomal recessive inheritance pattern -
 Alpha-mannosidosis
Alpha-mannosidosis -
 Alpha-mannosidosis electron micrograph
Alpha-mannosidosis electron micrograph



Sponsored Health Resource

W8MD Weight Loss, Sleep & MedSpa
Looking for physician-supervised weight loss, semaglutide, tirzepatide, or GLP-1 receptor agonist options? W8MD helps eligible patients in New York City, Brooklyn, New Jersey, Connecticut, Pennsylvania, Delaware, and greater Philadelphia with medical weight loss, sleep medicine, and long-term maintenance support.
GLP-1 specials: Affordable GLP-1 injections NYC and Philadelphia starting from $29.99/week and up for semaglutide with insurance accepted for qualifying visits, and $45/week and up for tirzepatide with insurance accepted for qualifying visits. Self-pay options start from $59.99/week and up for semaglutide and $69.99/week and up for tirzepatide.
- Medical weight loss NYC
- Affordable GLP-1 injections NYC
- Budget GLP-1 weight loss shots Philadelphia
- New Jersey medical weight loss
- NYC medical weight loss blog
- Philadelphia weight loss blog
- Sleep medicine and sleep apnea services
- W8MD MedSpa and wellness
Book a W8MD appointment · View GLP-1 specials
Paid promotional message. Eligibility, pricing, insurance coverage, medication availability, and results vary. Medical evaluation required.

Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian
