Cardiac catheterization
| Pronunciation | |
|---|---|
| Other names | |
| Specialty | |
| Uses | |
| Complications | |
| Approach | |
| Types | |
| Recovery time | |
| Other options | |
| Frequency |
Cardiac catheterization is a medical procedure used to diagnose and treat certain cardiovascular conditions. During this procedure, a long thin tube called a catheter is inserted in an artery or vein in your groin, neck, or arm and threaded through your blood vessels to your heart.
Indications[edit]
Cardiac catheterization is used to investigate and treat a variety of heart conditions, including:
Procedure[edit]
The procedure is typically performed in a catheterization laboratory (cath lab) by a cardiologist and a specialized team of nurses and technicians. The patient is usually awake but sedated, and local anesthesia is applied to the insertion site.
Steps[edit]
1. **Preparation**: The patient is prepared and the insertion site is cleaned and numbed. 2. **Insertion**: A sheath is inserted into the blood vessel. 3. **Catheterization**: The catheter is guided through the blood vessels to the heart using fluoroscopy. 4. **Diagnosis and Treatment**: Various tests and treatments can be performed, such as angiography, angioplasty, or stent placement. 5. **Completion**: The catheter and sheath are removed, and pressure is applied to the insertion site to prevent bleeding.
Risks[edit]
While cardiac catheterization is generally safe, it does carry some risks, including:
Recovery[edit]
After the procedure, patients are monitored for several hours. They may need to lie flat for a few hours to prevent bleeding from the insertion site. Most patients can return to normal activities within a few days.
See also[edit]
References[edit]
External links[edit]
Cardiac catheterization[edit]
-
 Cardiac catheterization
Cardiac catheterization -
Radial artery catheterization
-
 Left Heart Catheter
Left Heart Catheter -
Pulmonary artery Catheter
-
 X-ray of pacemaker with right atrial and ventricular lead
X-ray of pacemaker with right atrial and ventricular lead -
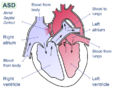 Atrial septal defect
Atrial septal defect -
 Takotsubo ventriculography
Takotsubo ventriculography






Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian

{kind=link}
{kind=link}