Membranoproliferative glomerulonephritis
| Membranoproliferative glomerulonephritis | |
|---|---|
| Membranoproliferative glomerulonephritis - very high mag.jpg | |
| Synonyms | N/A |
| Pronounce | N/A |
| Specialty | N/A |
| Symptoms | N/A |
| Complications | N/A |
| Onset | N/A |
| Duration | N/A |
| Types | N/A |
| Causes | N/A |
| Risks | N/A |
| Diagnosis | N/A |
| Differential diagnosis | N/A |
| Prevention | N/A |
| Treatment | N/A |
| Medication | N/A |
| Prognosis | N/A |
| Frequency | N/A |
| Deaths | N/A |
Membranoproliferative glomerulonephritis (MPGN), also known as mesangiocapillary glomerulonephritis, is a type of glomerulonephritis characterized by alterations in the glomerular basement membrane, mesangial cell proliferation, and changes in the glomerular capillary walls. It is a rare kidney disorder that can lead to chronic kidney disease.
Pathophysiology[edit]
MPGN is primarily caused by immune complex deposition in the glomeruli, leading to inflammation and structural changes. The disease is classified into three types based on the location and nature of these deposits:
- Type I MPGN: Characterized by subendothelial immune complex deposits. It is often associated with infections such as hepatitis C and hepatitis B, as well as autoimmune diseases like systemic lupus erythematosus.
- Type II MPGN: Also known as dense deposit disease, it involves dense deposits within the glomerular basement membrane. This type is linked to abnormalities in the complement system, particularly the alternative pathway.
- Type III MPGN: Features both subendothelial and subepithelial deposits. It is less common and its pathogenesis is not as well understood.
Clinical Presentation[edit]
Patients with MPGN may present with a variety of symptoms, including:
- Hematuria (blood in urine)
- Proteinuria (protein in urine)
- Hypertension (high blood pressure)
- Edema (swelling)
- Reduced kidney function
Diagnosis[edit]
Diagnosis of MPGN is typically confirmed through a kidney biopsy, which reveals the characteristic histological changes. Immunofluorescence microscopy can help identify the type of immune deposits present.
Treatment[edit]
Treatment of MPGN depends on the underlying cause and may include:
- Immunosuppressive therapy (e.g., corticosteroids, cyclophosphamide)
- Antiviral therapy for associated infections
- Blood pressure control
- Management of complications such as chronic kidney disease
Prognosis[edit]
The prognosis of MPGN varies. Some patients may experience a slow progression to end-stage renal disease, while others may have a more stable course. Early diagnosis and treatment can improve outcomes.
Also see[edit]
References[edit]
-
 Membranoproliferative glomerulonephritis
Membranoproliferative glomerulonephritis -
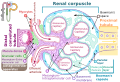 Renal corpuscle diagram
Renal corpuscle diagram



Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian
