Nerve injury classification
Nerve injury classification refers to the system used to categorize nerve injuries based on the extent of damage to the nerve and its surrounding structures. This classification system is crucial in determining the appropriate treatment and predicting the prognosis of nerve injuries.
Types of Nerve Injuries[edit]
Nerve injuries are classified into three main types: neurapraxia, axonotmesis, and neurotmesis.
Neurapraxia[edit]
Neurapraxia is the mildest form of nerve injury. It is characterized by a temporary blockage of nerve conduction, often due to compression or mild trauma. The nerve structure remains intact, and recovery is usually complete.
Axonotmesis[edit]
Axonotmesis involves more severe damage, with disruption of the nerve axon and myelin sheath but preservation of the connective tissue framework (the endoneurium). This type of injury often results from crush injuries or severe compression, and recovery may be partial or complete, depending on the extent of the damage and the effectiveness of treatment.
Neurotmesis[edit]
Neurotmesis is the most severe type of nerve injury, involving complete disruption of the nerve and its surrounding connective tissue. This type of injury is usually the result of severe trauma, such as a cut or tear, and recovery is generally poor.
Seddon's Classification[edit]
British neurologist Sydney Sunderland further expanded the classification of nerve injuries into five degrees, based on the severity of the injury and the structures involved. This is often referred to as Seddon's classification.
Sunderland's Classification[edit]
Sunderland's classification system further divides axonotmesis into three separate grades (second, third, and fourth degree injuries), and neurotmesis as a fifth degree injury. This classification provides a more detailed prognosis and guides the treatment plan.
Treatment and Prognosis[edit]
The treatment and prognosis of nerve injuries depend on the type and severity of the injury. Mild injuries often recover fully with conservative management, while severe injuries may require surgical intervention and have a poorer prognosis.
See Also[edit]
| Nervous system | ||||
|---|---|---|---|---|
|

This WikiMD article can only be edited by registered and verified editors. You can log in or register.
Nerve injury classification[edit]
-
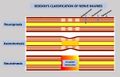 Sedon's classification of nerve injuries
Sedon's classification of nerve injuries

Sponsored Health Resource

W8MD Weight Loss, Sleep & MedSpa
Looking for physician-supervised weight loss, semaglutide, tirzepatide, or GLP-1 receptor agonist options? W8MD helps eligible patients in New York City, Brooklyn, New Jersey, Connecticut, Pennsylvania, Delaware, and greater Philadelphia with medical weight loss, sleep medicine, and long-term maintenance support.
GLP-1 specials: Affordable GLP-1 injections NYC and Philadelphia starting from $29.99/week and up for semaglutide with insurance accepted for qualifying visits, and $45/week and up for tirzepatide with insurance accepted for qualifying visits. Self-pay options start from $59.99/week and up for semaglutide and $69.99/week and up for tirzepatide.
- Medical weight loss NYC
- Affordable GLP-1 injections NYC
- Budget GLP-1 weight loss shots Philadelphia
- New Jersey medical weight loss
- NYC medical weight loss blog
- Philadelphia weight loss blog
- Sleep medicine and sleep apnea services
- W8MD MedSpa and wellness
Book a W8MD appointment · View GLP-1 specials
Paid promotional message. Eligibility, pricing, insurance coverage, medication availability, and results vary. Medical evaluation required.

Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian
