Acute interstitial pneumonitis
| Acute interstitial pneumonitis | |
|---|---|
 | |
| Synonyms | Hamman–Rich syndrome |
| Pronounce | N/A |
| Specialty | Pulmonology |
| Symptoms | Cough, dyspnea, fever |
| Complications | Respiratory failure, acute respiratory distress syndrome |
| Onset | Sudden |
| Duration | Days to weeks |
| Types | N/A |
| Causes | Unknown, possibly viral infection or autoimmune disease |
| Risks | Smoking, viral infections, autoimmune disorders |
| Diagnosis | Chest X-ray, CT scan, lung biopsy |
| Differential diagnosis | Acute respiratory distress syndrome, pneumonia, pulmonary embolism |
| Prevention | N/A |
| Treatment | Supportive care, mechanical ventilation, corticosteroids |
| Medication | N/A |
| Prognosis | Poor, high mortality rate |
| Frequency | Rare |
| Deaths | N/A |

Acute interstitial pneumonitis (AIP), also known as Hamman-Rich syndrome, is a rare and severe form of interstitial lung disease characterized by the rapid onset of respiratory failure. It is classified as an idiopathic form of diffuse alveolar damage (DAD) and is considered a type of acute respiratory distress syndrome (ARDS).
Pathophysiology[edit]
AIP is characterized by diffuse alveolar damage, which involves injury to the alveolar epithelium and capillary endothelium. This leads to the formation of hyaline membranes, interstitial edema, and infiltration of inflammatory cells. The exact cause of AIP is unknown, but it is thought to be triggered by an acute inflammatory response in the lungs.
Clinical presentation[edit]
Patients with AIP typically present with sudden onset of dyspnea, cough, and fever. The condition progresses rapidly to severe respiratory failure, often requiring mechanical ventilation. The clinical course is similar to that of ARDS, but AIP is distinguished by its idiopathic nature and histological findings.
Diagnosis[edit]
The diagnosis of AIP is based on clinical presentation, imaging studies, and histopathological examination. High-resolution computed tomography (HRCT) of the chest often shows diffuse bilateral ground-glass opacities and consolidation. A lung biopsy is usually required to confirm the diagnosis, revealing the characteristic diffuse alveolar damage with hyaline membrane formation.
Treatment[edit]
There is no specific treatment for AIP, and management is primarily supportive. Patients often require mechanical ventilation and intensive care. Corticosteroids and other immunosuppressive agents may be used, but their efficacy is uncertain. The prognosis is generally poor, with a high mortality rate.
Prognosis[edit]
The prognosis of AIP is poor, with a high mortality rate, often exceeding 50%. Survivors may experience long-term pulmonary sequelae, including pulmonary fibrosis.
Related pages[edit]
- Interstitial lung disease
- Acute respiratory distress syndrome
- Diffuse alveolar damage
- Pulmonary fibrosis
Gallery[edit]
-
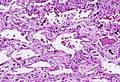 Histopathological image showing diffuse alveolar damage
Histopathological image showing diffuse alveolar damage -
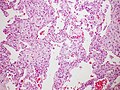
 Another view of diffuse alveolar damage in AIP
Another view of diffuse alveolar damage in AIP -
 Diffuse alveolar damage with hyaline membranes
Diffuse alveolar damage with hyaline membranes
_Idiopathic_DAD_3.jpg)
_Idiopathic_DAD_2.jpg)
_Idiopathic_DAD.jpg)

Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian
