Cranial root of accessory nerves
Cranial root of accessory nerves refers to a component of the accessory nerve, also known as the eleventh cranial nerve (CN XI), which is unique among the cranial nerves because it has both a cranial and a spinal root. The cranial root of the accessory nerve arises from the medulla oblongata, which is part of the brainstem, and it is primarily involved in the motor function of certain muscles in the neck and shoulder.
Anatomy[edit]
The cranial root of the accessory nerve originates from the nucleus ambiguus in the medulla oblongata. This nucleus is also responsible for giving rise to the motor fibers of the vagus nerve (CN X). The fibers of the cranial root exit the skull through the jugular foramen, along with the vagus and spinal accessory nerves. After exiting the skull, the cranial root joins the spinal root of the accessory nerve. The combined nerve then travels to innervate the sternocleidomastoid and trapezius muscles, which are vital for head movement and shoulder elevation.
Function[edit]
The primary function of the cranial root of the accessory nerve is motor control. It contributes to the movement of the pharynx and larynx, which are essential for swallowing and vocalization, through its integration with the vagus nerve. This is because the fibers of the cranial root eventually merge with the vagus nerve and distribute motor fibers to the muscles of the larynx and pharynx.
Clinical Significance[edit]
Damage to the accessory nerve, including its cranial root, can result in a range of symptoms depending on the location of the injury. Such symptoms may include weakness or paralysis of the sternocleidomastoid and trapezius muscles, leading to difficulties in head movement and shoulder elevation. Additionally, since the cranial root contributes to the motor function of the pharynx and larynx, damage can also affect swallowing and speech.
Diagnosis of accessory nerve damage often involves physical examination and may be supported by imaging studies such as MRI or CT scans. Treatment depends on the underlying cause of the damage and may include physical therapy to strengthen the affected muscles or surgical intervention in some cases.
See Also[edit]
This neuroscience article is a stub. You can help WikiMD by expanding the page. |
-
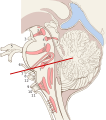 Sagittal section of the brain stem
Sagittal section of the brain stem -
 Cranial root of accessory nerves
Cranial root of accessory nerves


Sponsored Health Resource

W8MD Weight Loss, Sleep & MedSpa
Looking for physician-supervised weight loss, semaglutide, tirzepatide, or GLP-1 receptor agonist options? W8MD helps eligible patients in New York City, Brooklyn, New Jersey, Connecticut, Pennsylvania, Delaware, and greater Philadelphia with medical weight loss, sleep medicine, and long-term maintenance support.
GLP-1 specials: Affordable GLP-1 injections NYC and Philadelphia starting from $29.99/week and up for semaglutide with insurance accepted for qualifying visits, and $45/week and up for tirzepatide with insurance accepted for qualifying visits. Self-pay options start from $59.99/week and up for semaglutide and $69.99/week and up for tirzepatide.
- Medical weight loss NYC
- Affordable GLP-1 injections NYC
- Budget GLP-1 weight loss shots Philadelphia
- New Jersey medical weight loss
- NYC medical weight loss blog
- Philadelphia weight loss blog
- Sleep medicine and sleep apnea services
- W8MD MedSpa and wellness
Book a W8MD appointment · View GLP-1 specials
Paid promotional message. Eligibility, pricing, insurance coverage, medication availability, and results vary. Medical evaluation required.

Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian
