Acute lymphoblastic leukemia
| Acute Lymphoblastic Leukemia | |
|---|---|
| Synonyms | Acute lymphocytic leukemia, acute lymphoid leukemia |
| Pronounce | N/A |
| Specialty | Oncology, Hematology |
| Symptoms | Fever, bleeding, bone pain, fatigue |
| Complications | Infection, Anemia, bleeding |
| Onset | |
| Duration | |
| Types | |
| Causes | Genetic mutations, environmental factors |
| Risks | Radiation exposure, genetic disorders |
| Diagnosis | Blood tests, bone marrow biopsy |
| Differential diagnosis | |
| Prevention | |
| Treatment | Chemotherapy, radiation therapy, stem cell transplant |
| Medication | |
| Prognosis | Varies by age and genetic factors |
| Frequency | |
| Deaths | |
Acute lymphoblastic leukemia (ALL) is a type of cancer that affects the white blood cells. It is characterized by the overproduction of immature white blood cells, known as lymphoblasts or leukemic blasts. ALL is most commonly diagnosed in children, making it the most prevalent type of cancer in this age group, but it can also affect adults.
Etiology[edit]
The exact cause of ALL is not well understood, but it is believed to involve a combination of genetic and environmental factors. Genetic mutations in the DNA of bone marrow cells can lead to the development of ALL. These mutations cause the cells to grow uncontrollably and accumulate, leading to leukemia. Environmental factors, such as exposure to radiation or toxic chemicals, may also play a role in the development of ALL.
Pathophysiology[edit]
In ALL, the genetic mutations affect the lymphoid line of blood cells, leading to the production of abnormal lymphoblasts. These cells are unable to function properly as immune cells and rapidly divide, crowding out normal blood cells in the bone marrow. This disruption in blood cell production leads to the symptoms associated with ALL, such as anemia, infection, and bleeding disorders.
Symptoms[edit]
Common symptoms of ALL include:
- Fever
- Frequent infections
- Fatigue
- Bleeding and bruising easily
- Bone and joint pain
- Swollen lymph nodes
- Abdominal discomfort due to an enlarged spleen or liver
Diagnosis[edit]
Diagnosis of ALL typically involves blood tests, which may show an abnormal number of white blood cells and a presence of blast cells. A bone marrow biopsy is often performed to confirm the diagnosis and to determine the specific type of leukemia.
Treatment[edit]
Treatment for ALL usually involves a combination of therapies including:
- Chemotherapy: the main treatment for ALL, which uses drugs to kill cancer cells.
- Radiation therapy: sometimes used to kill cancer cells or to prepare for a stem cell transplant.
- Stem cell transplant: replaces diseased bone marrow with healthy bone marrow from a donor.
Treatment may vary depending on the patient's age, overall health, and specific characteristics of the leukemia.
Prognosis[edit]
The prognosis for patients with ALL varies. Children often have a better prognosis than adults, with higher rates of remission and cure. The prognosis in adults is influenced by the specific subtype of ALL and the presence of certain genetic abnormalities.
Epidemiology[edit]
ALL is the most common type of cancer in children and represents a significant percentage of cancer diagnoses in this group. It is less common in adults, but the incidence increases with age.
See also[edit]
This medical article is a stub. You can help WikiMD by expanding the page. |
-
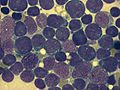
Morphological types of acute lymphoblastic leukemia
-
 Diagram showing the cell that ALL starts in
Diagram showing the cell that ALL starts in -
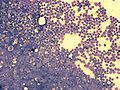
 ALL - Peripheral Blood - Diagnosis
ALL - Peripheral Blood - Diagnosis -
 Acute lymphoblastic leukemia
Acute lymphoblastic leukemia -
 Acute lymphoblastic leukemia
Acute lymphoblastic leukemia -
 Pediatric patients receiving chemotherapy
Pediatric patients receiving chemotherapy -
Overall survival rates in pediatric and adult ALL patients






Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian

{kind=link}
{kind=link}