Birt–Hogg–Dubé syndrome

Editor-In-Chief: Prab R Tumpati, MD
Obesity, Sleep & Internal medicine
Founder, WikiMD Wellnesspedia &
W8MD's weight loss doctor NYC
Philadelphia GLP-1 weight loss and GLP-1 clinic NYC
| Birt–Hogg–Dubé syndrome | |
|---|---|

| |
| Synonyms | BHD, Hornstein–Knickenberg syndrome |
| Pronounce | |
| Specialty | Dermatology, Genetics |
| Symptoms | Fibrofolliculomas, trichodiscomas, acrochordons, pulmonary cysts, spontaneous pneumothorax, renal tumors |
| Complications | Renal cell carcinoma |
| Onset | Typically in adulthood |
| Duration | Chronic |
| Types | |
| Causes | Mutations in the FLCN gene |
| Risks | Family history of the condition |
| Diagnosis | Genetic testing, clinical examination |
| Differential diagnosis | Tuberous sclerosis, neurofibromatosis |
| Prevention | |
| Treatment | Surveillance, surgical removal of tumors |
| Medication | |
| Prognosis | Generally good with management |
| Frequency | Rare |
| Deaths | |
Birt–Hogg–Dubé syndrome (BHD) is a rare genetic disorder that is associated with skin lesions, lung disease, and kidney tumors. It is named after the three scientists who first described the condition in 1977: Arthur R. Birt, Georgina R. Hogg, and Dr. William J. Dubé.
Symptoms and Signs[edit]
The symptoms of Birt–Hogg–Dubé syndrome can vary greatly from person to person. Some people may have only skin abnormalities, while others may also have lung and kidney problems. The skin lesions associated with BHD are often flesh-colored and can appear anywhere on the body, but they are most commonly found on the face, neck, and upper body. People with BHD are also at an increased risk of developing certain types of kidney cancer. These tumors usually develop in adulthood and can be either benign (noncancerous) or malignant (cancerous).
Causes[edit]
Birt–Hogg–Dubé syndrome is caused by mutations in the Folliculin (FLCN) gene. This gene provides instructions for making a protein that is involved in regulating cell growth and division. Mutations in the FLCN gene lead to the production of an abnormal folliculin protein, which disrupts the normal regulation of cell growth and division. This can lead to the formation of tumors and cysts in the skin, lungs, and kidneys.
Diagnosis[edit]
The diagnosis of Birt–Hogg–Dubé syndrome is based on a clinical evaluation, detailed patient history, and a variety of specialized tests. These tests may include a skin biopsy to examine the skin lesions, imaging tests such as a CT scan or MRI to look for lung and kidney abnormalities, and genetic testing to identify mutations in the FLCN gene.
Treatment[edit]
There is currently no cure for Birt–Hogg–Dubé syndrome. Treatment is aimed at managing the symptoms and preventing complications. This may include surgery to remove skin lesions or kidney tumors, medications to manage lung disease, and regular monitoring to detect any new tumors or cysts.
Gallery[edit]
-
 Birt–Hogg–Dubé syndrome
Birt–Hogg–Dubé syndrome -
 Birt–Hogg–Dubé syndrome
Birt–Hogg–Dubé syndrome -
Histopathology of chromophobe renal cell carcinoma
-
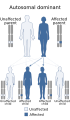 Autosomal dominant inheritance pattern
Autosomal dominant inheritance pattern -
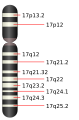 Chromosome 17
Chromosome 17 -
 Patient with facial angiofibromas caused by tuberous sclerosis
Patient with facial angiofibromas caused by tuberous sclerosis





See Also[edit]
References[edit]
- Birt AR, Hogg GR, Dubé WJ. Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch Dermatol. 1977 Dec;113(12):1674-7.
- Toro JR, Glenn G, Duray P, et al. Birt-Hogg-Dubé syndrome: a novel marker of kidney neoplasia. Arch Dermatol. 1999 Oct;135(10):1195-202.


Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian

{kind=link}