Alagille syndrome
| Alagille syndrome | |
|---|---|
| Autosomal dominant - en.svg | |
| Alagille syndrome is inherited in an autosomal dominant manner | |
| Synonyms | Alagille–Watson syndrome (ALGS), hepatic ductular hypoplasia
|
Alagille syndrome is a genetic disorder that affects multiple organ systems, primarily the liver, heart, eyes, skeleton, and kidneys. It is characterized by a paucity of intrahepatic bile ducts, leading to cholestasis and other systemic manifestations.
Etiology[edit]
Alagille syndrome is primarily caused by mutations in the JAG1 gene, which encodes a ligand in the Notch signaling pathway. In some cases, mutations in the NOTCH2 gene are also implicated. These mutations are typically inherited in an autosomal dominant pattern, although de novo mutations can occur.
Pathophysiology[edit]
The Notch signaling pathway plays a crucial role in cell differentiation and organ development. Mutations in JAG1 or NOTCH2 disrupt this pathway, leading to the characteristic features of Alagille syndrome. The paucity of bile ducts results in impaired bile flow, causing cholestasis and subsequent liver damage.
Clinical Features[edit]
Hepatic Manifestations[edit]
The most prominent feature of Alagille syndrome is cholestasis, which often presents in infancy. Patients may exhibit jaundice, pruritus, and xanthomas. Progressive liver disease can lead to cirrhosis and liver failure.
Cardiac Anomalies[edit]
Congenital heart defects are common, with pulmonary artery stenosis being the most frequent. Other possible anomalies include tetralogy of Fallot and ventricular septal defect.
Skeletal Abnormalities[edit]
Characteristic skeletal findings include butterfly vertebrae, which are often asymptomatic but can be detected on X-ray.
Ocular Features[edit]
Patients may have posterior embryotoxon, a thickened and anteriorly displaced Schwalbe's line visible on slit-lamp examination.
Renal Involvement[edit]
Renal abnormalities can include renal tubular acidosis and other structural anomalies.
Diagnosis[edit]
Diagnosis of Alagille syndrome is based on clinical criteria and confirmed by genetic testing. A liver biopsy may show bile duct paucity, supporting the diagnosis. Genetic testing can identify mutations in JAG1 or NOTCH2.
Management[edit]
Management of Alagille syndrome is primarily supportive and symptomatic. Treatment options include:
- Ursodeoxycholic acid to improve bile flow.
- Cholestyramine or rifampicin for pruritus.
- Nutritional support, including fat-soluble vitamin supplementation.
- Liver transplantation in cases of end-stage liver disease.
Prognosis[edit]
The prognosis of Alagille syndrome varies depending on the severity of organ involvement. Liver disease is a major determinant of outcome, and some patients may require liver transplantation. Cardiac anomalies may also impact prognosis.
Epidemiology[edit]
Alagille syndrome occurs in approximately 1 in 30,000 to 45,000 live births. It affects both males and females equally.
See Also[edit]
References[edit]
- Kamath BM, et al. "Alagille syndrome: diagnosis and management." Clin Liver Dis. 2018.
- McDaniell R, et al. "NOTCH2 mutations cause Alagille syndrome, a heterogeneous disorder of the notch signaling pathway." Am J Hum Genet. 2006.
| Congenital malformations and deformations of digestive system | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| Diseases of cilia | ||||||
|---|---|---|---|---|---|---|
See also: ciliary proteins
|

This WikiMD article can only be edited by registered and verified editors. You can log in or register.
Alagille syndrome[edit]
-
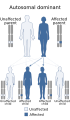 Autosomal dominant inheritance pattern
Autosomal dominant inheritance pattern -
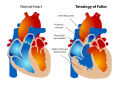 Tetralogy of Fallot
Tetralogy of Fallot


Sponsored Health Resource

W8MD Weight Loss, Sleep & MedSpa
Looking for physician-supervised weight loss, semaglutide, tirzepatide, or GLP-1 receptor agonist options? W8MD helps eligible patients in New York City, Brooklyn, New Jersey, Connecticut, Pennsylvania, Delaware, and greater Philadelphia with medical weight loss, sleep medicine, and long-term maintenance support.
GLP-1 specials: Affordable GLP-1 injections NYC and Philadelphia starting from $29.99/week and up for semaglutide with insurance accepted for qualifying visits, and $45/week and up for tirzepatide with insurance accepted for qualifying visits. Self-pay options start from $59.99/week and up for semaglutide and $69.99/week and up for tirzepatide.
- Medical weight loss NYC
- Affordable GLP-1 injections NYC
- Budget GLP-1 weight loss shots Philadelphia
- New Jersey medical weight loss
- NYC medical weight loss blog
- Philadelphia weight loss blog
- Sleep medicine and sleep apnea services
- W8MD MedSpa and wellness
Book a W8MD appointment · View GLP-1 specials
Paid promotional message. Eligibility, pricing, insurance coverage, medication availability, and results vary. Medical evaluation required.

Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian
