The Humerus
Anatomy > Gray's Anatomy of the Human Body > II. [Osteology]] > 6a. 3. The Humerus
Henry Gray (1821–1865). Anatomy of the Human Body. 1918.
The Humerus[edit]
(Arm Bone)
The humerus (Figs. 207, 208) is the longest and largest bone of the upper extremity; it is divisible into a body and two extremities
Upper Extremity[edit]
The upper extremity consists of a large rounded head joined to the body by a constricted portion called the neck and two eminences, the greater and lesser tubercles
The Head (caput humeri)[edit]
The head, nearly hemispherical in form, 54 is directed upward, medialward, and a little backward, and articulates with the glenoid cavity of the scapula. The circumference of its articular surface is slightly constricted and is termed the anatomical neck in contradistinction to a constriction below the tubercles called the surgical neck which is frequently the seat of fracture.
Fracture of the anatomical neck rarely occurs. The Anatomical Neck (collum anatomicum) is obliquely directed, forming an obtuse angle with the body. It is best marked in the lower half of its circumference; in the upper half it is represented by a narrow groove separating the head from the tubercles. It affords attachment to the articular capsule of the shoulder-joint, and is perforated by numerous vascular foramina.
The Greater Tubercle (tuberculum majus; greater tuberosity)[edit]
The greater tubercle is situated lateral to the head and lesser tubercle. Its upper surface is rounded and marked by three flat impressions: the highest of these gives insertion to the Supraspinatus; the middle to the Infraspinatus; the lowest one, and the body of the bone for about 2.5 cm. below it, to the Teres minor. The lateral surface of the greater tubercle is convex, rough, and continuous with the lateral surface of the body.
The Lesser Tubercle (tuberculum minus; lesser tuberosity)[edit]
The lesser tubercle, although smaller, is more prominent than the greater: it is situated in front, and is directed medialward and forward. Above and in front it presents an impression for the insertion of the tendon of the Subscapularis.
The tubercles are separated from each other by a deep groove, the intertubercular groove (bicipital groove), which lodges the long tendon of the Biceps brachii and transmits a branch of the anterior humeral circumflex artery to the shoulder-joint. It runs obliquely downward, and ends near the junction of the upper with the middle third of the bone.
In the fresh state its upper part is covered with a thin layer of cartilage, lined by a prolongation of the synovial membrane of the shoulder-joint; its lower portion gives insertion to the tendon of the Latissimus dorsi. It is deep and narrow above, and becomes shallow and a little broader as it descends. Its lips are called, respectively, the crests of the greater and lesser tubercles (bicipital ridges), and form the upper parts of the anterior and medial borders of the body of the bone.
The Body or Shaft (corpus humeri)[edit]
The body is almost cylindrical in the upper half of its extent, prismatic and flattened below, and has three borders and three surfaces.
Borders[edit]
The anterior border runs from the front of the greater tubercle above to the coronoid fossa below, separating the antero-medial from the antero-lateral surface. Its upper part is a prominent ridge, the crest of the greater tubercle; it serves for the insertion of the tendon of the Pectoralis major. About its center it forms the anterior boundary of the deltoid tuberosity; below, it is smooth and rounded, affording attachment to the Brachialis.
The lateral border runs from the back part of the greater tubercle to the lateral epicondyle, and separates the anterolateral from the posterior surface. Its upper half is rounded and indistinctly marked, serving for the attachment of the lower part of the insertion of the Teres minor, and below this giving origin to the lateral head of the Triceps brachii; its center is traversed by a broad but shallow oblique depression, the radial sulcus (musculospiral groove). Its lower part forms a prominent, rough margin, a little curved from behind forward, the lateral supracondylar ridge which presents an anterior lip for the origin of the Brachioradialis above, and Extensor carpi radialis longus below, a posterior lip for the Triceps brachii, and an intermediate ridge for the attachment of the lateral intermuscular septum.
FIG. 207– Left humerus. Anterior view. (Picture From the Classic Gray's Anatomy)
The medial border extends from the lesser tubercle to the medial epicondyle. Its upper third consists of a prominent ridge, the crest of the lesser tubercle which gives insertion to the tendon of the Teres major. About its center is a slight impression for the insertion of the Coracobrachialis, and just below this is the entrance of the nutrient canal, directed downward; sometimes there is a second nutrient canal at the commencement of the radial sulcus.
The inferior third of this border is raised into a slight ridge, the medial supracondylar ridge which becomes very prominent below; it presents an anterior lip for the origins of the Brachialis and Pronator teres, a posterior lip for the medial head of the Triceps brachii, and an intermediate ridge for the attachment of the medial intermuscular septum.
Surfaces[edit]
The antero-lateral surface is directed lateralward above, where it is smooth, rounded, and covered by the Deltoideus; forward and lateralward below, where it is slightly concave from above downward, and gives origin to part of the Brachialis. About the middle of this surface is a rough, triangular elevation, the deltoid tuberosity for the insertion of the Deltoideus; below this is the radial sulcus directed obliquely from behind, forward, and downward, and transmitting the radial nerve and profunda artery.
FIG. 208– Left humerus. Posterior view. (Picture From the Classic Gray's Anatomy)
The antero-medial surface less extensive than the antero-lateral, is directed medialward above, forward and medialward below; its upper part is narrow, and forms the floor of the intertubercular groove which gives insertion to the tendon of the Latissimus dorsi; its middle part is slightly rough for the attachment of some of the fibers of the tendon of insertion of the Coracobrachialis; its lower part is smooth, concave from above downward, and gives origin to the Brachialis.
The posterior surface appears somewhat twisted, so that its upper part is directed a little medialward, its lower part backward and a little lateralward. Nearly the whole of this surface is covered by the lateral and medial heads of the Triceps brachii, the former arising above, the latter below the radial sulcus.
The Lower Extremity[edit]
The lower extremity is flattened from before backward, and curved slightly forward; it ends below in a broad, articular surface, which is divided into two parts by a slight ridge. Projecting on either side are the lateral and medial epicondyles.
The articular surface extends a little lower than the epicondyles, and is curved slightly forward; its medial extremity occupies a lower level than the lateral. The lateral portion of this surface consists of a smooth, rounded eminence, named the capitulum of the humerus it articulates with the cupshaped depression on the head of the radius, and is limited to the front and lower part of the bone.
On the medial side of this eminence is a shallow groove, in which is received the medial margin of the head of the radius. Above the front part of the capitulum is a slight depression, the radial fossa which receives the anterior border of the head of the radius, when the forearm is flexed. The medial portion of the articular surface is named the trochlea and presents a deep depression between two well-marked borders; it is convex from before backward, concave from side to side, and occupies the anterior, lower, and posterior parts of the extremity.
The lateral border separates it from the groove which articulates with the margin of the head of the radius. The medial border is thicker, of greater length, and consequently more prominent, than the lateral. The grooved portion of the articular surface fits accurately within the semilunar notch of the ulna; it is broader and deeper on the posterior than on the anterior aspect of the bone, and is inclined obliquely downward and forward toward the medial side.
Above the front part of the trochlea is a small depression, the coronoid fossa which receives the coronoid process of the ulna during flexion of the forearm. Above the back part of the trochlea is a deep triangular depression, the olecranon fossa in which the summit of the olecranon is received in extension of the forearm. These fossae are separated from one another by a thin, transparent lamina of bone, which is sometimes perforated by a supratrochlear foramen they are lined in the fresh state by the synovial membrane of the elbow-joint, and their margins afford attachment to the anterior and posterior ligaments of this articulation.
The lateral epicondyle is a small, tuberculated eminence, curved a little forward, and giving attachment to the radial collateral ligament of the elbow-joint, and to a tendon common to the origin of the Supinator and some of the Extensor muscles.
The medial epicondyle larger and more prominent than the lateral, is directed a little backward; it gives attachment to the ulnar collateral ligament of the elbow-joint, to the Pronator teres, and to a common tendon of origin of some of the Flexor muscles of the forearm; the ulnar nerve runs in a groove on the back of this epicondyle. The epicondyles are continuous above with the supracondylar ridges.
Structure[edit]
The extremities consist of cancellous tissue, covered with a thin, compact layer (Fig. 209); the body is composed of a cylinder of compact tissue, thicker at the center than toward the extremities, and contains a large medullary canal which extends along its whole length.
Ossification (Figs. 210, 211)[edit]
The humerus is ossified from eight centers, one for each of the following parts: the body, the head, the greater tubercle, the lesser tubercle, the capitulum, the trochlea, and one for each epicondyle. The center for the body appears near the middle of the bone in the eighth week of fetal life, and soon extends toward the extremities.
At birth the humerus is ossified in nearly its whole length, only the extremities remaining cartilaginous. During the first year, sometimes before birth, ossification commences in the head of the bone, and during the third year the center for the greater tubercle, and during the fifth that for the lesser tubercle, make their appearance.
By the sixth year the centers for the head and tubercles have joined, so as to form a single large epiphysis, which fuses with the body about the twentieth year. The lower end of the humerus is ossified as follows. At the end of the second year ossification begins in the capitulum, and extends medialward, to form the chief part of the articular end of the bone; the center for the medial part of the trochlea appears about the age of twelve.
Ossification begins in the medial epicondyle about the fifth year, and in the lateral about the thirteenth or fourteenth year. About the sixteenth or seventeenth year, the lateral epicondyle and both portions of the articulating surface, having already joined, unite with the body, and at the eighteenth year the medial epicondyle becomes joined to it.
FIG. 209– Longitudinal section of head of left humerus. (Picture From the Classic Gray's Anatomy)
FIG. 210– Plan of ossification of the humerus. (Picture From the Classic Gray's Anatomy)
FIG. 211– Epiphysial lines of humerus in a young adult. Anterior aspect. The lines of attachment of the articular capsules are in blue. (Picture From the Classic Gray's Anatomy)
Note 54 Though the head is nearly hemispherical in form, its margin, as Humphry has shown, is by no means a true circle. Its greatest diameter is, from the top of the intertubercular groove in a direction downward, medialward, and backward. Hence it follows that the greatest elevation of the arm can be obtained by rolling the articular surface in this direction—that is to say, obliquely upward, lateralward, and forward.
Note 55 A small, hook-shaped process of bone, the supracondylar process varying from 2 to 20 mm. in length, is not infrequently found projecting from the antero-medial surface of the body of the humerus 5 cm. above the medial epicondyle. It is curved downward and forward, and its pointed end is connected to the medial border, just above the medial epicondyle, by a fibrous band, which gives origin to a portion of the Pronator teres; through the arch completed by this fibrous band the median nerve and brachial artery pass, when these structures deviate from their usual course.
Sometimes the nerve alone is transmitted through it, or the nerve may be accompanied by the ulnar artery, in cases of high division of the brachial. A well-marked groove is usually found behind the process, in which the nerve and artery are lodged. This arch is the homologue of the supracondyloid foramen found in many animals, and probably serves in them to protect the nerve and artery from compression during the contraction of the muscles in this region.
Additional images[edit]
-
Position of humerus (shown in red). Animation.
-
Left humerus. Animation.
-
3D image
-
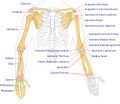 Human arm bones diagram.
Human arm bones diagram. -
Humerus - inferior epiphysis. Anterior view.
-
Trochlea. Posterior view.
-
Humerus - inferior epiphysis. Posterior view.
-
Humerus - superior epiphysis. Anterior view.
-
Humerus - superior epiphysis. Posterior view.
-
 Elbow joint. Deep dissection. Anterior view.
Elbow joint. Deep dissection. Anterior view. -
 Elbow joint. Deep dissection. Posterior view.
Elbow joint. Deep dissection. Posterior view. -
 Elbow joint. Deep dissection. Posterior view.
Elbow joint. Deep dissection. Posterior view.

.jpg)


External links[edit]
- Humerus - BlueLink Anatomy, University of Michigan Medical School
| Bones of the arm | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Gray's Anatomy[edit]
- Gray's Anatomy Contents
- Gray's Anatomy Subject Index
- About Classic Gray's Anatomy
- Glossary of anatomy terms
Anatomy atlases (external)[edit]
[1] - Anatomy Atlases
| Human systems and organs | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Sponsored Health Resource

W8MD Weight Loss, Sleep & MedSpa
Looking for physician-supervised weight loss, semaglutide, tirzepatide, or GLP-1 receptor agonist options? W8MD helps eligible patients in New York City, Brooklyn, New Jersey, Connecticut, Pennsylvania, Delaware, and greater Philadelphia with medical weight loss, sleep medicine, and long-term maintenance support.
GLP-1 specials: Affordable GLP-1 injections NYC and Philadelphia starting from $29.99/week and up for semaglutide with insurance accepted for qualifying visits, and $45/week and up for tirzepatide with insurance accepted for qualifying visits. Self-pay options start from $59.99/week and up for semaglutide and $69.99/week and up for tirzepatide.
- Medical weight loss NYC
- Affordable GLP-1 injections NYC
- Budget GLP-1 weight loss shots Philadelphia
- New Jersey medical weight loss
- NYC medical weight loss blog
- Philadelphia weight loss blog
- Sleep medicine and sleep apnea services
- W8MD MedSpa and wellness
Book a W8MD appointment · View GLP-1 specials
Paid promotional message. Eligibility, pricing, insurance coverage, medication availability, and results vary. Medical evaluation required.

Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}