Diffuse panbronchiolitis

Editor-In-Chief: Prab R Tumpati, MD
Obesity, Sleep & Internal medicine
Founder, WikiMD Wellnesspedia &
W8MD's weight loss doctor NYC
Philadelphia GLP-1 weight loss and GLP-1 clinic NYC
| Diffuse panbronchiolitis | |
|---|---|

| |
| Synonyms | N/A |
| Pronounce | N/A |
| Specialty | N/A |
| Symptoms | Cough, sputum production, dyspnea |
| Complications | Bronchiectasis, respiratory failure |
| Onset | Typically in adulthood |
| Duration | Chronic |
| Types | N/A |
| Causes | Unknown, possibly genetic and environmental factors |
| Risks | Asian descent, particularly Japanese |
| Diagnosis | HRCT, pulmonary function tests |
| Differential diagnosis | Bronchiectasis, chronic obstructive pulmonary disease |
| Prevention | N/A |
| Treatment | Macrolide antibiotics, corticosteroids |
| Medication | N/A |
| Prognosis | Improved with treatment, but can lead to chronic respiratory failure |
| Frequency | Rare, more common in East Asia |
| Deaths | N/A |
Diffuse Panbronchiolitis (DPB) is a chronic inflammatory lung disease primarily affecting the bronchioles. It is characterized by chronic sinusitis, productive cough, and dyspnea. The condition is most commonly observed in individuals of East Asian descent, particularly in Japan and Korea.
Epidemiology[edit]
Diffuse Panbronchiolitis is predominantly seen in East Asian populations, with a higher prevalence in Japan. The disease is rare in other ethnic groups. The exact prevalence is not well-documented, but it is considered a rare disease outside of Asia.
Etiology[edit]
The exact cause of Diffuse Panbronchiolitis is unknown. However, there is a strong association with certain genetic markers, particularly the HLA-B54 antigen, suggesting a genetic predisposition. Environmental factors have not been clearly identified.
Pathophysiology[edit]
The disease is characterized by chronic inflammation of the bronchioles, leading to the formation of lymphoid follicles and infiltration of neutrophils and lymphocytes. This results in obstruction of the small airways and impaired mucociliary clearance, contributing to chronic infection and bronchiectasis.
Clinical Features[edit]
Patients with Diffuse Panbronchiolitis typically present with:
- Chronic cough
- Sputum production
- Dyspnea on exertion
- Chronic sinusitis
As the disease progresses, patients may develop respiratory failure and cor pulmonale.
Diagnosis[edit]
The diagnosis of Diffuse Panbronchiolitis is based on clinical evaluation, imaging studies, and sometimes lung biopsy.
Imaging[edit]
A CT scan of the chest typically shows diffuse nodular opacities and bronchiectasis, particularly in the lower lobes.
Biopsy[edit]
A lung biopsy may be performed to confirm the diagnosis, showing characteristic histopathological features such as lymphoid hyperplasia and inflammatory cell infiltration.
Treatment[edit]
The mainstay of treatment for Diffuse Panbronchiolitis is long-term macrolide antibiotic therapy, such as erythromycin or clarithromycin. These antibiotics have anti-inflammatory properties that help reduce airway inflammation and improve symptoms.
Prognosis[edit]
With appropriate treatment, the prognosis for patients with Diffuse Panbronchiolitis has improved significantly. Long-term macrolide therapy can lead to stabilization or improvement of lung function and symptoms.
Diffuse panbronchiolitis images[edit]
-
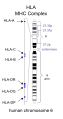 HLA
HLA -
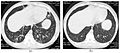 Diffuse panbronchiolitis
Diffuse panbronchiolitis -
 Erythromycin A
Erythromycin A



See Also[edit]
External Links[edit]
- WikiMD: Diffuse Panbronchiolitis
| Pulmonology topics | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
This pulmonology-related article is a stub. You can help WikiMD by expanding it.
|
| Respiratory diseases | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
This respiratory disease-related article is a stub.
|

Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian
