Central neurocytoma
A rare type of brain tumor
| Central neurocytoma | |
|---|---|
| Neurocytome axiale.jpg | |
| Axial T1-weighted gadolinium-enhanced MRI image showing an enhancing mass with cystic changes consistent with central neurocytoma in the right lateral ventricle. | |
| Synonyms | Intraventricular neurocytoma
|
| Specialty | Oncology, neurosurgery, neuropathology |
| Symptoms | Headache, nausea, vomiting, visual disturbances, hydrocephalus, seizures |
| Complications | Obstructive hydrocephalus, recurrence, postoperative complications |
| Usual onset | Typically in young adults (20–40 years) |
| Duration | Chronic, may recur |
| Types | Central and extraventricular neurocytoma |
| Causes | Unknown; believed to be related to neuronal progenitor cells |
| Risk factors | No clear environmental or genetic risk factors identified |
| Diagnosis | MRI, CT scan, biopsy, histopathology with immunohistochemical markers (e.g., synaptophysin positive) |
| Differential diagnosis | Ependymoma, oligodendroglioma, subependymal giant cell astrocytoma, choroid plexus papilloma |
| Prevention | None known |
| Treatment | Surgical resection (gross total or subtotal), radiation therapy for residual or recurrent tumors |
| Medication | Not typically used; symptomatic treatment for increased intracranial pressure |
| Prognosis | Generally good with complete resection; 5-year survival ~80–90% |
| Frequency | Rare; accounts for <1% of all brain tumors |
| Deaths | Rare with proper treatment |
Central neurocytoma is a rare brain tumor that typically arises in the ventricular system of the central nervous system. It is considered a neuroepithelial tumor and is most commonly found in young adults.
Presentation[edit]
Central neurocytomas are usually located in the lateral ventricles near the foramen of Monro. Patients often present with symptoms related to increased intracranial pressure, such as headache, nausea, and vomiting. Other symptoms may include vision problems, seizures, and cognitive changes.
Pathology[edit]
Central neurocytomas are classified as WHO Grade II tumors, indicating a low-grade malignancy. Histologically, they are composed of small, round cells with uniform nuclei and a moderate amount of cytoplasm. The tumor cells often form clusters and rosettes, resembling oligodendrogliomas. The presence of synaptophysin positivity on immunohistochemistry is a characteristic feature.
Diagnosis[edit]
The diagnosis of central neurocytoma is typically made through a combination of neuroimaging and histopathological examination. Magnetic resonance imaging (MRI) is the preferred imaging modality, often revealing a well-circumscribed mass in the ventricular system. Computed tomography (CT) scans may show calcifications within the tumor.
Treatment[edit]
The primary treatment for central neurocytoma is surgical resection. Complete removal of the tumor is often curative, but in cases where total resection is not possible, radiotherapy may be considered. The role of chemotherapy is limited and not well established.
Prognosis[edit]
The prognosis for patients with central neurocytoma is generally favorable, especially when the tumor is completely resected. The recurrence rate is low, and long-term survival is common. However, incomplete resection may lead to recurrence, necessitating further treatment.
Gallery[edit]
-
 High mag.
High mag. -
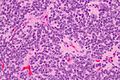 Very high mag.
Very high mag.


Related pages[edit]
External links[edit]
| Tumours of the nervous system | ||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Note: Not all brain tumors are of nervous tissue, and not all nervous tissue tumors are in the brain (see brain metastasis).
|

Sponsored Health Resource

W8MD Weight Loss, Sleep & MedSpa
Looking for physician-supervised weight loss, semaglutide, tirzepatide, or GLP-1 receptor agonist options? W8MD helps eligible patients in New York City, Brooklyn, New Jersey, Connecticut, Pennsylvania, Delaware, and greater Philadelphia with medical weight loss, sleep medicine, and long-term maintenance support.
GLP-1 specials: Affordable GLP-1 injections NYC and Philadelphia starting from $29.99/week and up for semaglutide with insurance accepted for qualifying visits, and $45/week and up for tirzepatide with insurance accepted for qualifying visits. Self-pay options start from $59.99/week and up for semaglutide and $69.99/week and up for tirzepatide.
- Medical weight loss NYC
- Affordable GLP-1 injections NYC
- Budget GLP-1 weight loss shots Philadelphia
- New Jersey medical weight loss
- NYC medical weight loss blog
- Philadelphia weight loss blog
- Sleep medicine and sleep apnea services
- W8MD MedSpa and wellness
Book a W8MD appointment · View GLP-1 specials
Paid promotional message. Eligibility, pricing, insurance coverage, medication availability, and results vary. Medical evaluation required.

Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian
