Shoulder
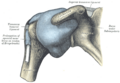
The synovial joint where the humerus joins the scapula
Anatomy > Gray's Anatomy of the Human Body > IV. Myology > 7c. The Muscles and Fasciæ of the Shoulder
Henry Gray (1821–1865). Anatomy of the Human Body. 1918.
The Muscles and Fasciæ of the Shoulder
In this group are included:
Deep Fascia—The deep fascia covering the Deltoideus invests the muscle, and sends numerous septa between its fasciculi. In front it is continuous with the fascia covering the Pectoralis major; behind, where it is thick and strong, with that covering the Infraspinatus; above, it is attached to the clavicle, the acromion, and the spine of the scapula; below, it is continuous with the deep fascia of the arm. The Deltoideus (Deltoid muscle) (Fig. 410) is a large, thick, triangular muscle, which covers the shoulder-joint in front, behind, and laterally.
It arises from the anterior border and upper surface of the lateral third of the clavicle; from the lateral margin and upper surface of the acromion, and from the lower lip of the posterior border of the spine of the scapula, as far back as the triangular surface at its medial end. From this extensive origin the fibers converge toward their insertion, the middle passing vertically, the anterior obliquely backward and lateralward, the posterior obliquely forward and lateralward; they unite in a thick tendon, which is inserted into the deltoid prominence on the middle of the lateral side of the body of the humerus.
At its insertion the muscle gives off an expansion to the deep fascia of the arm. This muscle is remarkably coarse in texture, and the arrangement of its fibers is somewhat peculiar; the central portion of the muscle—that is to say, the part arising from the acromion—consists of oblique fibers; these arise in a bipenniform manner from the sides of the tendinous intersections, generally four in number, which are attached above to the acromion and pass downward parallel to one another in the substance of the muscle. The oblique fibers thus formed are inserted into similar tendinous intersections, generally three in number, which pass upward from the insertion of the muscle and alternate with the descending septa. The portions of the muscle arising from the clavicle and spine of the scapula are not arranged in this manner, but are inserted into the margins of the inferior tendon.
Variations—Large variations uncommon. More or less splitting common. Continuation into the Trapezius; fusion with the Pectoralis major; additional slips from the vertebral border of the scapula, infraspinous fascia and axillary border of scapula not uncommon. Insertion varies in extent or rarely is prolonged to origin of Brachioradialis.
Nerves—The Deltoideus is supplied by the fifth and sixth cervical through the axillary nerve.
Actions—The Deltoideus raises the arm from the side, so as to bring it at right angles with the trunk. Its anterior fibers, assisted by the Pectoralis major, draw the arm forward; and its posterior fibers, aided by the Teres major and Latissimus dorsi, draw it backward.
Subscapular Fascia (fascia subscapularis)—The subscapular fascia is a thin membrane attached to the entire circumference of the subscapular fossa, and affording attachment by its deep surface to some of the fibers of the Subscapularis.
The Subscapularis (Fig. 411) is a large triangular muscle which fills the subscapular fossa, and arises from its medial two-thirds and from the lower two-thirds of the groove on the axillary border of the bone. Some fibers arise from tendinous laminæ which intersect the muscle and are attached to ridges on the bone; others from an aponeurosis, which separates the muscle from the Teres major and the long head of the Triceps brachii. The fibers pass lateralward, and, gradually converging, end in a tendon which is inserted into the lesser tubercle of the humerus and the front of the capsule of the shoulder-joint. The tendon of the muscle is separated from the neck of the scapula by a large bursa, which communicates with the cavity of the shoulder-joint through an aperture in the capsule.
Nerves—The Subscapularis is supplied by the fifth and sixth cervical nerves through the upper and lower subscapular nerves.
Actions—The Subscapularis rotates the head of the humerus inward; when the arm is raised, it draws the humerus forward and downward. It is a powerful defence to the front of the shoulder-joint, preventing displacement of the head of the humerus.
Supraspinatous Fascia (fascia supraspinata)—The supraspinatous fascia completes the osseofibrous case in which the Supraspinatus muscle is contained; it affords attachment, by its deep surface, to some of the fibers of the muscle. It is thick medially, but thinner laterally under the coracoacromial ligament.
The Supraspinatus (Fig. 412) occupies the whole of the supraspinatous fossa, arising from its medial two-thirds, and from the strong supraspinatous fascia. The muscular fibers converge to a tendon, which crosses the upper part of the shoulder-joint, and is inserted into the highest of the three impressions on the greater tubercle of the humerus; the tendon is intimately adherent to the capsule of the shoulder-joint.
Infraspinatous Fascia (fascia infraspinata)—The infraspinatous fascia is a dense fibrous membrane, covering the Infraspinatous muscle and fixed to the circum ference of the infraspinatous fossa; it affords attachment, by its deep surface, to some fibers of that muscle. It is intimately attached to the deltoid fascia along the over-lapping border of the Deltoideus. 13
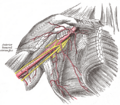
FIG. 412– —Muscles on the dorsum of the scapula, and the Triceps brachii. (Picture From the Classic Gray's Anatomy)
The Infraspinatus (Fig. 412) is a thick triangular muscle, which occupies the chief part of the infraspinatous fossa; it arises by fleshy fibers from its medial two-thirds, and by tendinous fibers from the ridges on its surface; it also arises from the infraspinatous fascia which covers it, and separates it from the Teretes major and minor. The fibers converge to a tendon, which glides over the lateral border of the spine of the scapula, and, passing across the posterior part of the capsule of the shoulder-joint, is inserted into the middle impression on the greater tubercle of the humerus. The tendon of this muscle is sometimes separated from the capsule of the shoulder-joint by a bursa, which may communicate with the joint cavity. 14
The Teres minor (Fig. 412) is a narrow, elongated muscle, which arises from the dorsal surface of the axillary border of the scapula for the upper two-thirds of its extent, and from two aponeurotic laminæ, one of which separates it from the Infraspinatus, the other from the Teres major. Its fibers run obliquely upward and lateralward; the upper ones end in a tendon which is inserted into the lowest of the three impressions on the greater tubercle of the humerus; the lowest fibers are inserted directly into the humerus immediately below this impression. The tendon of this muscle passes across, and is united with, the posterior part of the capsule of the shoulder-joint. 15
Variations—It is sometimes inseparable from the Infraspinatus. 16 The Teres major (Fig. 412) is a thick but somewhat flattened muscle, which arises from the oval area on the dorsal surface of the inferior angle of the scapula, and from the fibrous septa interposed between the muscle and the Teres minor and Infraspinatus; the fibers are directed upward and lateralward, and end in a flat tendon, about 5 cm. long, which is inserted into the crest of the lesser tubercle of the humerus. The tendon, at its insertion, lies behind that of the Latissimus dorsi, from which it is separated by a bursa, the two tendons being, however, united along their lower borders for a short distance. 17
Nerves—The Supraspinatus and Infraspinatus are supplied by the fifth and sixth cervical nerves through the suprascapular nerve; the Teres minor, by the fifth cervical, through the axillary; and the Teres major, by the fifth and sixth cervical, through the lowest subscapular. 18
Actions—The Supraspinatus assists the Deltoideus in raising the arm from the side of the trunk and fixes the head of the humerus in the glenoid cavity. The Infraspinatus and Teres minor rotate the head of the humerus outward; they also assist in carrying the arm backward. One of the most important uses of these three muscles is to protect the shoulder-joint, the Supraspinatus supporting it above, and the Infraspinatus and Teres minor behind. The Teres major assists the Latissimus dorsi in drawing the previously raised humerus downward and backward, and in rotating it inward; when the arm is fixed it may assist the Pectorales and the Latissimus dorsi in drawing the trunk forward. 19
Gray's Anatomy Contents | Gray's Anatomy Subject Index[edit]
| Human regional anatomy | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
| Joints and ligaments of the arm | ||||||||
|---|---|---|---|---|---|---|---|---|
|
| Muscles of the arm | ||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Shoulder[edit]
-
 Left shoulder
Left shoulder -
 Gray's Anatomy illustration 327
Gray's Anatomy illustration 327 -
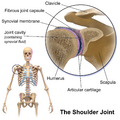 Blausen 0797 Shoulder Joint
Blausen 0797 Shoulder Joint -
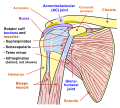 Shoulder joint
Shoulder joint -
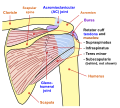 Shoulder joint back view
Shoulder joint back view -
 Gray's Anatomy illustration 523
Gray's Anatomy illustration 523 -
 Grant 1962 illustration 664
Grant 1962 illustration 664 -
 Gray's Anatomy illustrations 812 and 814
Gray's Anatomy illustrations 812 and 814 -
 Text-book of anatomy and physiology for nurses (1913)
Text-book of anatomy and physiology for nurses (1913) -
 Leonardo da Vinci - Anatomical studies of the shoulder
Leonardo da Vinci - Anatomical studies of the shoulder -
 Longitudinal ultrasound of supraspinatus
Longitudinal ultrasound of supraspinatus -
 Transversal ultrasound of supraspinatus
Transversal ultrasound of supraspinatus








_(14764575614).jpg)




Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian
