Coxal Articulation or Hip-joint

Editor-In-Chief: Prab R Tumpati, MD
Obesity, Sleep & Internal medicine
Founder, WikiMD Wellnesspedia &
W8MD's weight loss doctor NYC
Philadelphia GLP-1 weight loss and GLP-1 clinic NYC
Anatomy > Gray's Anatomy of the Human Body > III. Syndesmology > 7. Articulations of the Lower Extremity > Coxal Articulation or Hip-joint
Coxal Articulation or Hip-joint (Articulatio coxae)[edit]
The hip joint, or coxal articulation, is a synovial joint of the ball-and-socket (enarthrodial) type. It connects the lower limb to the pelvis and is formed by the articulation between the head of the femur and the acetabulum of the hip bone.
The joint allows a wide range of movements, including flexion, extension, abduction, adduction, rotation, and circumduction, while also providing significant stability due to its deep socket and strong surrounding ligaments and muscles.
Articulating Surfaces[edit]
- The head of the femur is covered with articular cartilage except at the fovea capitis femoris, where the ligamentum teres femoris attaches.
- The acetabulum is a deep, hemispherical cavity of the hip bone formed by the fusion of the ilium, ischium, and pubis.
- The acetabular surface is incomplete inferiorly due to the presence of the acetabular notch and features the lunate surface, which bears the weight of the body.
Ligaments of the Hip Joint[edit]
The joint is stabilized by several strong ligaments:
- Articular capsule (capsula articularis): Encloses the joint and attaches to the acetabulum and neck of femur.
- Iliofemoral ligament (ligamentum iliofemorale): Also known as the Y-ligament or ligament of Bigelow, one of the strongest ligaments in the body. Prevents hyperextension during standing.
- Pubofemoral ligament (ligamentum pubofemorale): Strengthens the capsule inferiorly and anteriorly.
- Ischiofemoral ligament (ligamentum ischiofemorale): Reinforces the posterior aspect of the capsule.
- Ligamentum teres femoris (ligament of head of femur): A weak ligament inside the joint that contains a branch of the obturator artery.
- Acetabular labrum (labrum acetabulare): A fibrocartilaginous rim that deepens the acetabular cavity.
- Transverse acetabular ligament: Bridges the acetabular notch and continues the labrum across the inferior part of the rim.
Synovial Membrane[edit]
The synovial membrane lines the inner surface of the capsule, covers the ligamentum teres, and reflects over the acetabular fat pad and acetabular fossa. It may communicate with the iliopsoas bursa.
Muscular Relations[edit]
Muscles surrounding the hip joint include:
- Anteriorly: Psoas major, Iliacus
- Posteriorly: Piriformis, Obturator internus, Gemelli, Quadratus femoris
- Laterally: Gluteus medius, Gluteus minimus
- Medially: Obturator externus, Pectineus
Blood Supply[edit]
The hip joint receives arterial supply from:
- Medial circumflex femoral artery
- Lateral circumflex femoral artery
- Obturator artery
- Superior gluteal artery
- Inferior gluteal artery
Innervation[edit]
The joint is innervated by branches of:
Movements[edit]
The hip joint allows:
- Flexion – by iliopsoas, rectus femoris, sartorius
- Extension – by gluteus maximus, hamstrings
- Abduction – by gluteus medius and gluteus minimus
- Adduction – by adductor longus, adductor brevis, adductor magnus, gracilis
- Lateral rotation – by obturator externus, piriformis, gluteus maximus
- Medial rotation – by tensor fasciae latae, gluteus minimus
Comparative Anatomy[edit]
Compared to the shoulder joint, the hip joint is more stable but less mobile. The deep acetabulum and strong ligaments enhance its load-bearing capacity.
Clinical Significance[edit]
- Hip fracture: Common in the elderly, often requiring hip replacement surgery.
- Hip dislocation: Typically caused by trauma, especially in motor vehicle accidents.
- Osteoarthritis of the hip: A degenerative condition causing pain and reduced mobility.
- Avascular necrosis: Disruption of blood supply to the femoral head, leading to joint destruction.
Additional Images[edit]
-
 Hip joint – lateral view
Hip joint – lateral view -
 Anterior thigh muscles related to hip joint
Anterior thigh muscles related to hip joint -
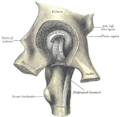 Hip joint opened from above
Hip joint opened from above -
 Muscular anatomy around hip joint
Muscular anatomy around hip joint -
 Hip anatomy (frontal view)
Hip anatomy (frontal view)





See Also[edit]
External Links[edit]
- Anatomy photo:21:st-2101 at the SUNY Downstate Medical Center
- MedlinePlus Encyclopedia: 002975
| Human regional anatomy | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
| Joints and ligaments of the human leg | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Gray's Anatomy[edit]
- Gray's Anatomy Contents
- Gray's Anatomy Subject Index
- About Classic Gray's Anatomy
- Glossary of anatomy terms
Anatomy atlases (external)[edit]
[1] - Anatomy Atlases
| Human systems and organs | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Adapted from the Classic Grays Anatomy of the Human Body 1918 edition (public domain)
Sponsored Health Resource

W8MD Weight Loss, Sleep & MedSpa
Looking for physician-supervised weight loss, semaglutide, tirzepatide, or GLP-1 receptor agonist options? W8MD helps eligible patients in New York City, Brooklyn, New Jersey, Connecticut, Pennsylvania, Delaware, and greater Philadelphia with medical weight loss, sleep medicine, and long-term maintenance support.
GLP-1 specials: Affordable GLP-1 injections NYC and Philadelphia starting from $29.99/week and up for semaglutide with insurance accepted for qualifying visits, and $45/week and up for tirzepatide with insurance accepted for qualifying visits. Self-pay options start from $59.99/week and up for semaglutide and $69.99/week and up for tirzepatide.
- Medical weight loss NYC
- Affordable GLP-1 injections NYC
- Budget GLP-1 weight loss shots Philadelphia
- New Jersey medical weight loss
- NYC medical weight loss blog
- Philadelphia weight loss blog
- Sleep medicine and sleep apnea services
- W8MD MedSpa and wellness
Book a W8MD appointment · View GLP-1 specials
Paid promotional message. Eligibility, pricing, insurance coverage, medication availability, and results vary. Medical evaluation required.

Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian
