Anemia

Editor-In-Chief: Prab R Tumpati, MD
Obesity, Sleep & Internal medicine
Founder, WikiMD Wellnesspedia &
W8MD's weight loss doctor NYC
Philadelphia GLP-1 weight loss and GLP-1 clinic NYC
| Anemia | |
|---|---|
 | |
| Synonyms | N/A |
| Pronounce | N/A |
| Specialty | N/A |
| Symptoms | Fatigue, weakness, shortness of breath, dizziness, palpitations |
| Complications | Heart failure, pregnancy complications, cognitive impairment |
| Onset | Gradual or sudden |
| Duration | Varies |
| Types | N/A |
| Causes | Iron deficiency, vitamin B12 deficiency, folate deficiency, chronic disease, genetic disorders |
| Risks | Poor diet, chronic diseases, family history, menstruation, pregnancy |
| Diagnosis | Complete blood count, blood smear, iron studies, bone marrow biopsy |
| Differential diagnosis | Thalassemia, sickle cell disease, hemolytic anemia |
| Prevention | Adequate nutrition, iron supplements, managing chronic conditions |
| Treatment | Iron supplements, vitamin B12 injections, folic acid supplements, blood transfusions |
| Medication | Erythropoiesis-stimulating agents, iron supplements |
| Prognosis | Varies depending on cause and treatment |
| Frequency | Common |
| Deaths | N/A |
Anemia (AmE)) or anaemia (BrE), from the Greek meaning "without blood", is a deficiency of red blood cells and/or hemoglobin. This results in a reduced ability of blood to transfer oxygen to the tissues, causing hypoxia; since all human cells depend on oxygen for survival, varying degrees of anemia can have a wide range of clinical consequences. Hemoglobin (the oxygen-carrying protein in the red blood cells) has to be present to ensure adequate oxygenation of all body tissues and organs. The three main classes of anemia include excessive blood loss (acutely such as a hemorrhage or chronically through low-volume loss), excessive blood cell destruction (hemolysis) or deficient red blood cell production. In menstruating women, dietary iron deficiency is a common cause of deficient red blood cell production. Anemia is the most common disorder of the blood. There are several kinds of anemia, produced by a variety of underlying causes. Anemia can be classified in a variety of ways, based on the morphology of RBCs, underlying etiologic mechanisms, and discernible clinical spectra, to mention a few. Different clinicians approach anemia in different ways; two major approaches of classifying anemias include the "kinetic" approach which involves evaluating production, destruction and loss, and the "morphologic" approach which groups anemia by red blood cell size. The morphologic approach uses a quickly available and cheap lab test as its starting point (the MCV). On the other hand, focusing early on the question of production (e.g., via the reticulocyte count) may allow the clinician more rapidly to expose cases where multiple causes of anemia coexist. Regardless of one's philosophy about the classification of anemia, however, any methodical clinical evaluation should yield equally good results.

Signs and symptoms[edit]
Anemia goes undetected in many people, and symptoms can be vague. Most commonly, people with anemia report a feeling of weakness or fatigue. People with more severe anemia sometimes report shortness of breath. Very severe anemia prompts the body to compensate by markedly increasing cardiac output, leading to palpitations and sweatiness; this process can lead to heart failure in elderly people. Pallor (pale skin and mucosal linings) is only notable in cases of severe anemia, and is therefore not a reliable sign.
Diagnosis[edit]
The only way to definitively diagnose most cases of anemia is with a blood test. Generally, clinicians order a full blood count. Apart from reporting the number of red blood cells and the hemoglobin level, the automatic counters also measure the size of the red blood cells by flow cytometry, which is an important tool in distinguishing between the causes of anemia. A visual examination of a blood smear can also be helpful in some cases, and is sometimes a necessity in regions of the world where automated analysis is less accessible. In modern counters, four parameters (RBC Count, hemoglobin concentration, MCV and RDW) are measured, allowing others (hematocrit, mean corpuscular hemoglobin and mean corpuscular hemoglobin concentration) to be calculated, and compared to values adjusted for age and sex. For males, the hemoglobin level that is suggestive of anemia is usually less than 13.0 g/dl, and for females, it is less than 12.0 g/dl. Depending on the clinical philosophy, whether the hospital's automated counter can immediately add it to the initial tests, and the clinicians' attitudes towards ordering tests, a reticulocyte count may be ordered either as part of the initial workup or during followup tests. This is a nearly direct measure of the bone marrow's capacity to produce new red blood cells, and is thus the most used method of evaluating the problem of production. This can be especially important in cases where both loss and a production problem may co-exist. Many physicians use the reticulocyte production index – a calculation of the ratio between the level of anemia and the extent to which the reticulocyte count has risen in response. Even in cases where an obvious source of loss exists, this helps evaluate whether the bone marrow will be able to compensate for the loss, and at what rate. When the cause is not obvious, clinicians use other tests to further distinguish the cause for anemia. These are discussed with the differential diagnosis, below. A clinician may also decide to order other screening blood tests that might identify the cause of fatigue; serum glucose, ESR, ferritin, serum iron, RBC folate level, serum vitamin B12, renal function tests (e.g. serum creatinine) and electrolytes may be part of such a workup.
Classification[edit]
The "kinetic" approach to anemia yields what many argue is the most clinically relevant classification of anemia. This classification depends on evaluation of several hematological parameters, particularly the blood reticulocyte (precursor of mature RBCs) count. This then yields the classification of defects by decreased RBC production, increased destruction, or blood loss. In the morphological approach, anemia is classified by the size of red blood cells; this is either done automatically or on microscopic examination of a peripheral blood smear. The size is reflected in the mean corpuscular volume (MCV). If the cells are smaller than normal (under 80 fl), the anemia is said to be microcytic; if they are normal size (80-100 fl), normocytic; and if they are larger than normal (over 100 fl), the anemia is classified as macrocytic. This scheme quickly exposes some of the most common causes of anemia; for instance, a microcytic anemia is often the result of iron deficiency. In clinical workup, the MCV will be one of the first pieces of information available; so even among clinicians who consider the "kinetic" approach more useful philosophically, morphology will remain an important element of classification and diagnosis. Other characteristics visible on the peripheral smear may provide valuable clues about a more specific diagnosis; for example, abnormal white blood cells may point to a cause in the bone marrow.
Microcytic anemia[edit]
- iron deficiency anemia is the most common type of anemia overall, and it is often hypochromic microcytic. Iron deficiency anemia is caused when the dietary intake or absorption of iron is insufficient. Iron is an essential part of hemoglobin, and low iron levels result in decreased incorporation of hemoglobin into red blood cells. In the United States, 20% of all women of childbearing age have iron deficiency anemia, compared with only 2% of adult men. The principal cause of iron deficiency anemia in premenopausal women is blood lost during menses. Studies have shown that iron deficiency without anemia causes poor school performance and lower IQ in teenage girls. In older patients, iron deficiency anemia is often due to bleeding lesions of the gastrointestinal tract; fecal occult blood testing, upper endoscopy and lower endoscopy are often performed to identify bleeding lesions, which can be malignant. Iron deficiency is the most prevalent deficiency state on a worldwide basis. Iron deficiency affects women from different cultures and ethnicities. In countries where meat consumption is not as common, iron deficiency anemia is six to eight times more prevalent than in North America and Europe. This is due to the importance of meat in the diets of North Americans and Europeans. A characteristic of iron deficiency is angular chelitis, which is an abnormal fissuring of the angular sections (corners of the mouth) of the lips.
- hemoglobinopathies -- much rarer (apart from communities where these conditions are prevalent)
Microcytic anemia is primarily a result of hemoglobin synthesis failure/insufficiency, which could be caused by several etiologies:
- Heme synthesis defect
- Iron deficiency
- Anemia of Chronic Disorders (which, sometimes, is grouped into normocytic anemia)
- Globin synthesis defect
- alpha-, and beta-thalassemia
- HbE syndrome
- HbC syndrome
- and various other unstable hemoglobin diseases
- Sideroblastic defect
- Hereditary Sideroblastic anemia
- Acquired Sideroblastic anemia
- Reversible Sideroblastic anemia
A mnemonic commonly used to remember causes of microcytic anemia is TAILS: T - Thalassemia, A - Anemia of chronic disease, I - Iron deficiency anemia, L - Lead toxicity associated anemia, S - Sideroblastic anemia.
Normocytic anemia[edit]
- Acute blood loss
- Anemia of chronic disease
- Aplastic anemia (bone marrow failure)
Macrocytic anemia[edit]
- Megaloblastic anemia due to a deficiency of either vitamin B12 or folic acid (or both) due either to inadequate intake or insufficient absorption. Folate deficiency normally does not produce neurological symptoms, while B12 deficiency does. Megaloblastic anemia is the most common cause of macrocytic anemia.
- Pernicious anemia is an autoimmune condition directed against the parietal cells of the stomach. Parietal cells produce intrinsic factor, required to absorb vitamin B12 from food. Therefore, the destruction of the parietal cells causes a lack of intrinsic factor, leading to poor absorption of vitamin B12.
- Alcoholism
- Methotrexate, zidovudine, and other drugs that inhibit DNA replication. This is the most common etiology in nonalcoholic patients.
Macrocytic anemia can be further divided into "megaloblastic anemia" or "non-megaloblastic macrocytic anemia". The cause of megaloblastic anemia is primarily a failure of DNA synthesis with preserved RNA synthesis, which result in restricted cell division of the progenitor cells. The megaloblastic anemias often present with neutrophil hypersegmentation (6-10 lobes). The non-megaloblastic macrocytic anemias have different etiologies (i.e. there is unimpaired DNA synthesis,) which occur, for example in alcoholism. The treatment for vitamin B12-deficient macrocytic and pernicious anemias was first devised by William Murphy who bled dogs to make them anemic and then fed them various substances to see what (if anything) would make them healthy again. He discovered that ingesting large amounts of liver seemed to cure the disease. George Minot and George Whipple then set about to chemically isolate the curative substance and ultimately were able to isolate the vitamin B12 from the liver. For this, all three shared the 1934 Nobel Prize in Medicine. Symptoms of vitamin B12 deficiency include having a smooth, red tongue.
Dimorphic anemia[edit]
Here there are two types of anemia simultaneously, e.g., macrocytic hypochromic, due to hookworm infestation leading to deficiency of both iron and vitamin B12 or folic acid [1] or following a blood transfusion.
Specific anemias[edit]
- Fanconi anemia is an hereditary disease featuring aplastic anemia and various other abnormalities
- Hemolytic anemia is a separate constellation of symptoms (also featuring jaundice and elevated LDH levels) with numerous potential causes. It can be autoimmune, immune, hereditary or mechanical (e.g. heart surgery). It can result (because of cell fragmentation) in a microcytic anemia, a normochromic anemia, or (because of premature release of immature red blood cells from the bone marrow), a macrocytic anemia.
- Hereditary spherocytosis is a hereditary disease that results in defects in the RBC cell membrane, causing the erythrocytes to be sequestered and destroyed by the spleen. This leads to a decrease in the number of circulating RBCs and, hence, anemia.
- Warm autoimmune hemolytic anemia is an anemia caused by autoimmune attack against red blood cells, primarily by IgM
Possible complications[edit]
Anemia diminishes the capability of individuals who are affected to perform physical labor. This is a result of one's muscles being forced to depend on anaerobic metabolism. The lack of iron associated with anemia can cause many complications, including hypoxemia, brittle or rigid fingernails, cold intolerance, impaired immune function, and possible behavioral disturbances in children. Hypoxemia resulting from anemia can worsen the cardio-pulmonary status of patients with pre-existing chronic pulmonary disease. Brittle or rigid fingernails may be a result of abnormal thinness of nails due to insufficient iron supply. Cold intolerance occurs in one in five patients with iron deficiency anemia, and becomes visible through numbness and tingling. Impaired immune functioning leading to increased likelihood of sickness is another possible complications. Finally, chronic anemia may result in behavioral disturbances in children as a direct result of impaired neurological development in infants, and reduced scholastic performance in children of school age. Behavioral disturbances may even surface as an attention deficit disorder.
Anemia during pregnancy[edit]
Anemia affects 20% of all females of childbearing age in the United States. Because of the subtlety of the symptoms, women are often unaware that they have this disorder, as they attribute the symptoms to the stresses of their daily lives. Possible problems for the fetus include increased risk of growth retardation, prematurity, intrauterine death, rupture of the amnion and infection. During pregnancy, women should be especially aware of the symptoms of anemia, as an adult female loses an average of two milligrams of iron daily. Therefore, she must intake a similar quantity of iron in order to make up for this loss. Additionally, a woman loses approximately 500 milligrams of iron with each pregnancy, compared to a loss of 4-100 milligrams of iron with each period. Possible consequences for the mother include cardiovascular symptoms, reduced physical and mental performance, reduced immune function, tiredness, reduced peripartal blood reserves and increased need for blood transfusion in the postpartum period.
Diet and anemia[edit]
Consumption of food rich in iron is essential to prevention of iron deficiency anemia; however, the average adult has approximately nine years worth of B12 stored in the liver, and it would take four to five years of an iron-deficient diet to create iron-deficiency anemia from diet alone. Iron-rich foods include red meat; green, leafy vegetables; dried beans; dried apricots, prunes, raisins, and other dried fruits; almonds; seaweeds; parsley; whole grains; and yams. In extreme cases of anemia, researchers recommend consumption of beef liver, lean meat, oysters, lamb or chicken, or iron drops may be introduced. Certain foods have been found to interfere with iron absorption in the gastrointestinal tract, and these foods should be avoided. They include tea, coffee, wheat bran, green leafy vegetables, rhubarb, chocolate, soft drinks, red wine, ice cream, and candy bars (Bauer, 2). With the exception of milk and eggs, animal sources of iron provide iron with better bioavailability than vegetable sources (Scrimshaw).
Treatments for anemia[edit]
There are many different treatments for anemia, including increasing dietary intake of readily available iron and iron supplementation; the treatment is determined by the type of anemia that is diagnosed. In severe cases of anemia, a blood transfusion may be necessary.
- Breymann, Christian. "Iron Deficiency and Anemia in Pregnancy: Modern Aspects of Diagnosis and Therapy." Blood Cells, Molecules, and Diseases. Nov/Dec: 2002.
- Conrad, Marcel E. "Iron Deficiency Anemia." EMedicine. 8 December 2004.
- Raymond, Tina. "Anemia: Diagnosis, Treatment and Prevention." Midwifery Today. 31 May 1999.
- Scrimshaw, Nevin. Iron deficiency. Scientific American Oct 1991 pp 46-52
- Schier, Stanley L. Approach to the adult patient with anemia. Up-to-Date (subscription required), accessed in Jan 2006, last changed June 2005.
- WHO Scientific Group on Nutritional Anaemias. "Nutritional anaemias : report of a WHO scientific group (meeting held in Geneva from 13 to 17 March 1967)". World Health Organization. Geneva, 1968.
See also[edit]
External links[edit]
- Iron Deficiency Anemia - emedicine.com
- Ambulatory Management of Common Forms of Anemia - American Academy of Family Physicians
- Anemia Lifeline
- National Anemia Action Council
Gallery[edit]
-
Blood Anemia
-
 DIC With Microangiopathic Hemolytic Anemia
DIC With Microangiopathic Hemolytic Anemia -
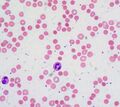
Iron-deficiency Anemia, Peripheral Blood Smear
-
 Warm autoimmune hemolytic anemia
Warm autoimmune hemolytic anemia -
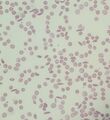
Dimorphic population of red blood cells
-
 Blood film of Hemoglobin SC disease
Blood film of Hemoglobin SC disease -
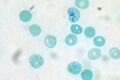 Reticulocytes Human Blood Supravital Stain
Reticulocytes Human Blood Supravital Stain -
 Sickle cell anemia smear
Sickle cell anemia smear -
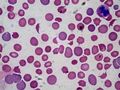
CLL with Autoimmune Hemolytic Anemia
-
Microangiopathic haemolytic anaemia





| Diseases of red blood cells | ||||
|---|---|---|---|---|
|

Sponsored Health Resource

W8MD Weight Loss, Sleep & MedSpa
Looking for physician-supervised weight loss, semaglutide, tirzepatide, or GLP-1 receptor agonist options? W8MD helps eligible patients in New York City, Brooklyn, New Jersey, Connecticut, Pennsylvania, Delaware, and greater Philadelphia with medical weight loss, sleep medicine, and long-term maintenance support.
GLP-1 specials: Affordable GLP-1 injections NYC and Philadelphia starting from $29.99/week and up for semaglutide with insurance accepted for qualifying visits, and $45/week and up for tirzepatide with insurance accepted for qualifying visits. Self-pay options start from $59.99/week and up for semaglutide and $69.99/week and up for tirzepatide.
- Medical weight loss NYC
- Affordable GLP-1 injections NYC
- Budget GLP-1 weight loss shots Philadelphia
- New Jersey medical weight loss
- NYC medical weight loss blog
- Philadelphia weight loss blog
- Sleep medicine and sleep apnea services
- W8MD MedSpa and wellness
Book a W8MD appointment · View GLP-1 specials
Paid promotional message. Eligibility, pricing, insurance coverage, medication availability, and results vary. Medical evaluation required.

Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian

{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
.jpg){kind=link}
.jpg){kind=link}