Alzheimer's disease

Editor-In-Chief: Prab R Tumpati, MD
Obesity, Sleep & Internal medicine
Founder, WikiMD Wellnesspedia &
W8MD's weight loss doctor NYC
Philadelphia GLP-1 weight loss and GLP-1 clinic NYC
| Alzheimer's disease | |
|---|---|

| |
| Synonyms | N/A |
| Pronounce | N/A |
| Specialty | N/A |
| Symptoms | Memory loss, confusion, difficulty with language, mood swings, disorientation |
| Complications | N/A |
| Onset | Usually after age 65 |
| Duration | Long term |
| Types | N/A |
| Causes | Genetics, age, environmental factors |
| Risks | Age, family history, genetic factors |
| Diagnosis | Cognitive testing, medical imaging |
| Differential diagnosis | Dementia with Lewy bodies, frontotemporal dementia, vascular dementia |
| Prevention | N/A |
| Treatment | Medications, supportive care |
| Medication | Acetylcholinesterase inhibitors, NMDA receptor antagonists |
| Prognosis | Progressive and incurable |
| Frequency | 50 million people worldwide (as of 2020) |
| Deaths | N/A |

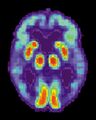
[[File:Alzheimers_Disease.jpg|Alzheimer's disease|thumb] Alzheimer's disease (AD) is a neurodegenerative disease characterized by progressive cognitive deterioration, declining activities of daily living, and neuropsychiatric symptoms or behavioral changes. It is the most common cause of dementia. The most striking early symptom is memory loss (amnesia), which usually manifests as minor forgetfulness that becomes more pronounced with illness progression, with relative preservation of older memories.
| Videos |
|---|
| Aging & Alzheimer's Disease, Part 1
Related Videos Aging & Alzheimer's Disease, Part 2 |
Symptoms and signs[edit]
As Alzheimer's disease progresses, cognitive impairment extends to various domains:
- Language (aphasia)
- Skilled movements (apraxia)
- Recognition (agnosia)
- Decision-making and planning, which are closely related to the frontal and temporal lobes of the brain as they become disconnected from the limbic system
Pathophysiology[edit]
The underlying pathological process in Alzheimer's disease consists mainly of neuronal loss or atrophy, accompanied by an inflammatory response to the deposition of amyloid plaques and neurofibrillary tangles.
Genetics[edit]
Genetic factors play a significant role in Alzheimer's disease. Autosomal dominant mutations in three different genes (presenilin 1, presenilin 2, and amyloid precursor protein) have been identified, accounting for a small number of cases of familial, early-onset AD. For late-onset AD (LOAD), only one susceptibility gene has been identified: the epsilon 4 allele of the apolipoprotein E gene. The age of onset itself has a heritability of around 50%.
Diagnosis[edit]
Diagnosis of Alzheimer's disease is typically based on a combination of medical history, physical examination, cognitive assessments, and imaging studies such as MRI and PET scans. Biomarker tests can also be used to support a diagnosis, but these are not yet widely available or validated for routine clinical use.
Treatment[edit]
Currently, there is no cure for Alzheimer's disease. Treatment focuses on managing symptoms and improving the quality of life for affected individuals. Medications such as cholinesterase inhibitors and memantine may help to alleviate cognitive symptoms. Supportive therapies, including occupational, physical, and speech therapy, can help maintain daily functioning and communication skills. Lifestyle modifications, such as regular exercise, a balanced diet, and adequate sleep, can help improve overall health and well-being.
Prognosis[edit]
Alzheimer's disease is a progressive disorder, with affected individuals experiencing a gradual decline in cognitive and functional abilities. The course of the disease can vary, with some people experiencing a more rapid progression than others. The average life expectancy after the onset of symptoms is approximately 8 to 10 years.
Gallery[edit]
-
Alzheimer's disease
-
 Alzheimer's disease
Alzheimer's disease -
 Alzheimer's disease
Alzheimer's disease -
 Alzheimer's disease
Alzheimer's disease



See also[edit]
- Dementia
- Lewy body dementia
- Parkinson's disease
- Neurodegenerative diseases
- Familial Alzheimer disease
- Dementia with Lewy bodies
- Frontotemporal lobar degeneration
- Corticobasal degeneration
- Memory and aging
- Memory loss
- Memory

This WikiMD article can only be edited by registered and verified editors. You can log in or register.
| Diseases of the nervous system, primarily CNS (G04–G47, 323–349) | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| Amyloidosis | ||||||
|---|---|---|---|---|---|---|
|
Sponsored Health Resource

W8MD Weight Loss, Sleep & MedSpa
Looking for physician-supervised weight loss, semaglutide, tirzepatide, or GLP-1 receptor agonist options? W8MD helps eligible patients in New York City, Brooklyn, New Jersey, Connecticut, Pennsylvania, Delaware, and greater Philadelphia with medical weight loss, sleep medicine, and long-term maintenance support.
GLP-1 specials: Affordable GLP-1 injections NYC and Philadelphia starting from $29.99/week and up for semaglutide with insurance accepted for qualifying visits, and $45/week and up for tirzepatide with insurance accepted for qualifying visits. Self-pay options start from $59.99/week and up for semaglutide and $69.99/week and up for tirzepatide.
- Medical weight loss NYC
- Affordable GLP-1 injections NYC
- Budget GLP-1 weight loss shots Philadelphia
- New Jersey medical weight loss
- NYC medical weight loss blog
- Philadelphia weight loss blog
- Sleep medicine and sleep apnea services
- W8MD MedSpa and wellness
Book a W8MD appointment · View GLP-1 specials
Paid promotional message. Eligibility, pricing, insurance coverage, medication availability, and results vary. Medical evaluation required.

Medical Disclaimer: WikiMD is for informational purposes only and is not a substitute for professional medical advice. Content may be inaccurate or outdated and should not be used for diagnosis or treatment. Always consult your healthcare provider for medical decisions. Verify information with trusted sources such as CDC.gov and NIH.gov. By using this site, you agree that WikiMD is not liable for any outcomes related to its content. See full disclaimer.
Credits:Most images are courtesy of Wikimedia commons, and templates, categories Wikipedia, licensed under CC BY SA or similar.
Translate page: - East Asian
中文,
日本,
한국어,
South Asian
हिन्दी,
தமிழ்,
తెలుగు,
Urdu,
ಕನ್ನಡ,
Southeast Asian
Indonesian,
Vietnamese,
Thai,
မြန်မာဘာသာ,
বাংলা
European
español,
Deutsch,
français,
Greek,
português do Brasil,
polski,
română,
русский,
Nederlands,
norsk,
svenska,
suomi,
Italian
Middle Eastern & African
عربى,
Turkish,
Persian,
Hebrew,
Afrikaans,
isiZulu,
Kiswahili,
Other
Bulgarian,
Hungarian,
Czech,
Swedish,
മലയാളം,
मराठी,
ਪੰਜਾਬੀ,
ગુજરાતી,
Portuguese,
Ukrainian

{kind=link}